

December 18, 2025
10 min
Ken Dawson
June 15, 2026
8 min

In 2002, the share of postmenopausal women using hormone therapy collapsed almost overnight — from roughly 27% to about 5% over the following years. One trial did that. Two decades later, reanalyses of that very same trial, plus the FDA itself in late 2025, have largely reversed the verdict. So what actually changed: the science, or the story we told about it?
What the evidence supports: For healthy women under 60 or within 10 years of menopause, hormone therapy is the most effective treatment for hot flashes and night sweats, prevents bone loss, and carries a favorable benefit-risk balance. The feared cardiovascular harm was largely an artifact of testing the therapy mostly in women in their 60s and 70s.
What’s overstated or unsupported: The blanket claim that estrogen “causes breast cancer and heart attacks” for everyone. Risk depends heavily on age, timing, formulation, dose, and route — and for estrogen-only therapy, breast cancer risk did not rise. Hormone therapy is also not a proven anti-aging or chronic-disease prevention tool for the general population.
⚕️ LyfeiQ Score: 8/10 — For the right candidate (symptomatic, recently menopausal, no contraindications), the evidence is now strong enough to have the conversation with a clinician rather than avoid it out of inherited fear.
The modern story of estrogen begins with a single 2002 headline that traveled faster than its own data. Through the 1980s and 1990s, observational studies and clinical enthusiasm had positioned hormone therapy as close to a preventive cure-all — good for bones, the heart, even cognition. Then came the Women’s Health Initiative (WHI), the largest randomized trial ever run on the question.
The combined estrogen-plus-progestin arm enrolled 16,608 women and was halted early in 2002 when an interim analysis crossed a safety boundary for breast cancer and showed the overall risk-benefit index tipping the wrong way (the WHI principal results, JAMA 2002). The reported hazard ratios — more coronary events, more strokes, more clots, more invasive breast cancer — were modest in absolute terms but landed like a thunderclap. Prescriptions cratered worldwide.
What got lost in the coverage: the average participant was 63 years old, more than a decade past menopause. The trial was designed to test chronic-disease prevention in older women, not symptom relief in women newly entering menopause. The estrogen-only arm, run in women with a prior hysterectomy, told a quieter and very different story — no increase in coronary heart disease and, if anything, a trend toward lower breast cancer risk (JAMA 2004). That nuance never made the headlines.
The reversal didn’t come from new ideology — it came from reanalyzing the same women by age. When investigators stratified the WHI data by how old participants were when they started therapy, a gradient appeared that the original top-line numbers had blurred.
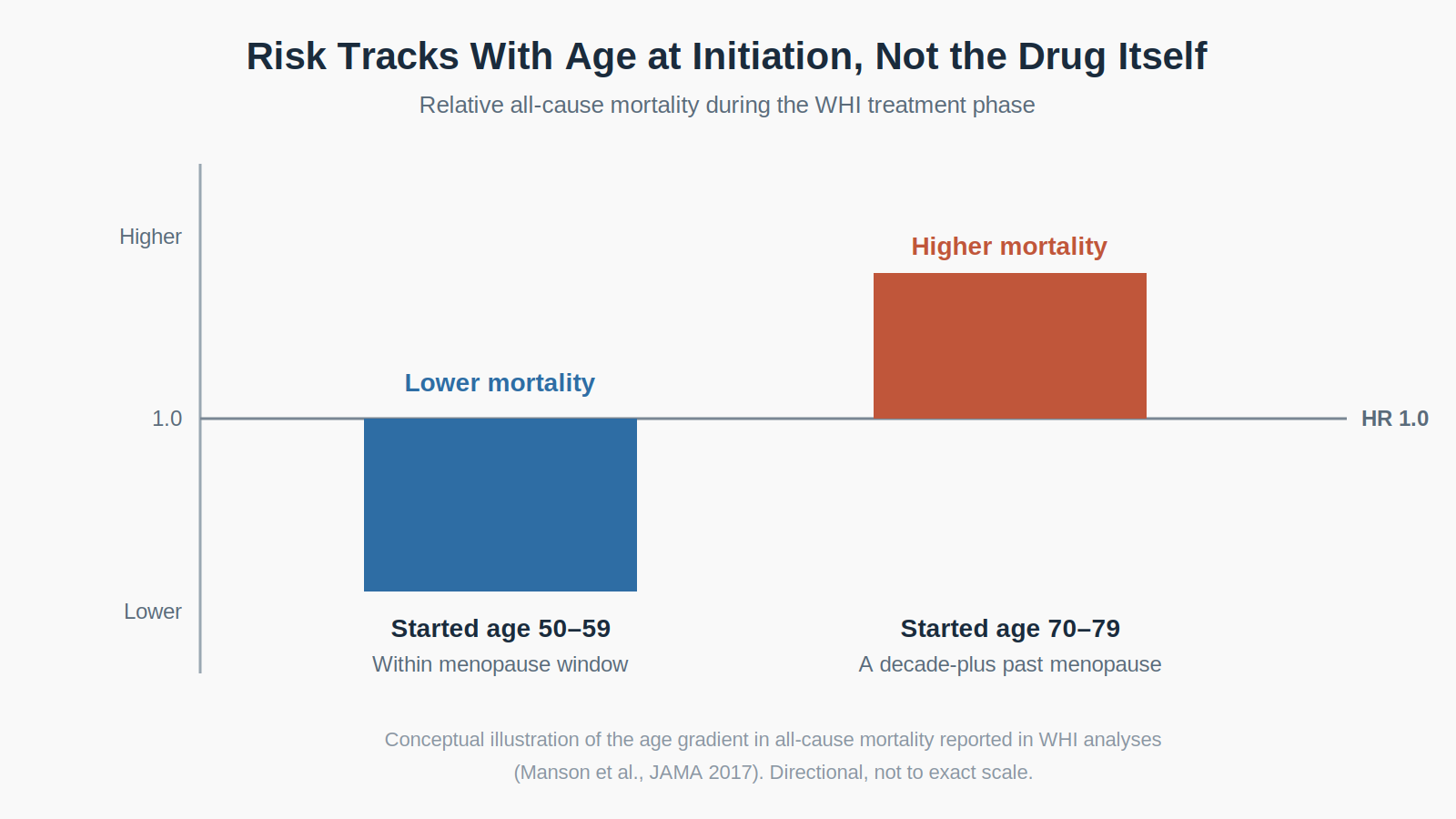
In the 18-year follow-up of both WHI hormone arms, hormone therapy was not associated with all-cause, cardiovascular, or cancer mortality (JAMA 2017). The much-feared death toll simply did not materialize over nearly two decades. And the ratio of mortality hazard for women who began in their 50s versus their 70s favored the younger starters during the treatment phase.
Then a purpose-built trial tested the idea head-on. The ELITE trial randomized 643 healthy postmenopausal women and deliberately split them by time since menopause. Among women less than six years out, oral estradiol slowed the progression of carotid-artery thickening compared with placebo; among women 10 or more years out, it didn’t (ELITE, New England Journal of Medicine 2016). Same drug, opposite vascular signal, depending entirely on when you start. Researchers call this the “timing hypothesis.”
A 2025 Cochrane review of 24 trials and 45,660 participants anchors the cautious side of the ledger: it confirms that combined therapy probably raises breast cancer risk and that both formulations raise stroke and clot risk, while reducing fractures — but notes that only about 30% of those women were in the 50–59 age band most likely to actually seek treatment today (Cochrane Database of Systematic Reviews, 2025). The evidence base, in other words, was built largely on women who aren’t the typical candidates.
The single most important variable is timing, and it’s one you partly control. Current clinical framing centers on a “window”: starting before age 60 or within 10 years of your final period is where the benefit-risk math is most favorable.
Formulation and route matter too. Transdermal estrogen (patches, gels) appears to carry lower clot and stroke risk than oral pills because it bypasses first-pass liver metabolism. Estradiol — chemically identical to the body’s own estrogen — is now far more commonly used than the conjugated equine estrogen the WHI tested. If you have a uterus, estrogen must be paired with a progestogen to protect the uterine lining. And low-dose vaginal estrogen, used for genitourinary symptoms, behaves almost like a different drug: its systemic absorption is minimal, and its risk profile is correspondingly low.
None of this is a do-it-yourself protocol. It’s a conversation to have with a clinician who treats menopause, ideally one who will individualize type, dose, route, and duration rather than reach for a single default.
Mainstream medical. Major bodies have converged. The Menopause Society’s 2022 position statement holds that for healthy symptomatic women under 60 or within 10 years of menopause, the benefits of hormone therapy outweigh the risks; the American College of Obstetricians and Gynecologists and the Endocrine Society align with that framing (menopause.org). Mainstream medicine still treats systemic estrogen as a prescription drug requiring individualized risk review — not a wellness accessory.
Alternative / integrative. Integrative practitioners often emphasize “body-identical” or bioidentical estradiol and progesterone, transdermal delivery, and lifestyle scaffolding (resistance training, protein, sleep, bone-loading exercise). Where regulated, FDA-approved bioidentical products are well supported; the contested edge is custom-compounded “bioidentical hormone replacement,” which lacks the same oversight and dosing consistency. Proponents make reasonable points about route and molecule that mainstream guidelines now partly echo.
Influencer / public. Menopause has become one of the most active corners of health social media, and popular creators — including physician-influencers who built large audiences advocating for hormone therapy access — have genuinely helped destigmatize a topic medicine neglected for years. The contrasting voice matters too: some oncologists and researchers caution that the online pendulum has swung toward overselling, treating estrogen as longevity insurance rather than a targeted symptom treatment. Both things can be true — the stigma was harmful, and the hype outruns the data.
The defensible claim and the oversold claim live very close together. The evidence strongly supports hormone therapy for bothersome vasomotor symptoms and bone protection in appropriately selected women, and it no longer supports the idea that estrogen is broadly dangerous for that group. The 2017 mortality data and the ELITE timing trial both point the same direction.
Where marketing gets ahead of science is the leap from “safe and effective for symptoms” to “essential for every woman’s healthy aging.” Hormone therapy is not FDA-approved to prevent heart disease or dementia, and the Cochrane data are a reminder that real risks — stroke, clots, gallbladder disease, and breast cancer with combined therapy — don’t vanish because the narrative improved. The honest synthesis: the original scare was overcorrected, and the current enthusiasm risks overcorrecting in the other direction.
Three threads are worth watching. First, the regulatory recalibration: in November 2025 the FDA announced it would remove the boxed warning from estrogen-containing products, with relabeling expected to carry age-specific guidance — a move that drew broad agreement for low-dose vaginal estrogen and more debate for systemic forms. Second, better-targeted trials in the 50–59 window, the group the foundational studies underrepresented. Third, the genuinely underexplored populations — women with premature or early menopause, where untreated estrogen deficiency carries its own long-term risks, and the basic question of optimal duration, which still rests on thin randomized evidence.
Credibility Rating: 8/10
👉 Who should try this: Women with bothersome hot flashes, night sweats, or genitourinary symptoms who are under 60 or within 10 years of menopause and have no contraindications — it’s worth a serious clinical conversation.
👉 Who should skip this: Women with a history of breast cancer, prior blood clots or stroke, active liver disease, or those well past the menopause window starting purely for prevention — here the balance shifts and alternatives deserve first look.
⚕️ LyfeiQ Score: 8/10 — If symptoms are disrupting your life and you’re in the window, don’t let a 2002 headline make the decision for you. Talk to a menopause-literate clinician about an individualized, likely transdermal, plan.
Related: The Collagen Paradox
Research sourced via PubMed.
Disclaimer: This content includes personal opinions and interpretations based on available sources and should not replace medical advice. This content includes interpretation of available research and should not replace medical advice. Although the data found in this blog and infographic has been produced and processed from sources believed to be reliable, no warranty expressed or implied can be made regarding the accuracy, completeness, legality or reliability of any such information. This disclaimer applies to any uses of the information whether isolated or aggregate uses thereof.

